Photo taken in Okayama, Japan
As a lay person, what I wish you all knew...
In traveling to many countries to engage in end of life issues and care, I came with the perspective of a patient or family member. Through this lens, I have been in absolute wonder at the caring, intelligent and skilled people I had the privilege to engage with, shadow, interview and observe. For all of you medical professionals, what I wish you all knew was how important you are, how you have such great opportunity to care for not just the body but the person. For better or for worse, end of life issues are becoming more medicalized but the potentialities that come along with this reality are so vast. I wish you knew that your involvement and decisions matter a great deal.
I wish you knew that your patients and their families know when you are or are not listening to us, we always see how you treat and engage with your colleagues, that all the basic human details matter, that taking the extra time to look us in the eye and be aware of our family dynamics is important, that honesty and hopelessness do not exactly go hand in hand: you can be honest without leaving us hopeless. I wish you knew that your compassion changes everything.
I know and have seen a great deal of problems in the medical systems around the world, there is no perfect system. You are up against so much and you are truly, truly heroes in my perspective, but by keeping the person always at the center not just by valuing your patients but by valuing your colleagues and treating them with respect, you not only humanize your patients and your families, but you uphold the dignity of all life and your very own profession. You have such an awesome responsibility and the good that you can do when you uphold this responsibility knows no bounds.
I wish you knew that your patients and their families know when you are or are not listening to us, we always see how you treat and engage with your colleagues, that all the basic human details matter, that taking the extra time to look us in the eye and be aware of our family dynamics is important, that honesty and hopelessness do not exactly go hand in hand: you can be honest without leaving us hopeless. I wish you knew that your compassion changes everything.
I know and have seen a great deal of problems in the medical systems around the world, there is no perfect system. You are up against so much and you are truly, truly heroes in my perspective, but by keeping the person always at the center not just by valuing your patients but by valuing your colleagues and treating them with respect, you not only humanize your patients and your families, but you uphold the dignity of all life and your very own profession. You have such an awesome responsibility and the good that you can do when you uphold this responsibility knows no bounds.
Creativity and Idea Generator
|
Idea
|
Where I saw this
(similar ideas or programs may be in other locations, I just may not have encounter it during my brief placement) |
Description
|
|
Coffee Shops
|
UK, Ireland, South Africa,
|
Many of the hospices have coffee shops run as an extension of their services. The coffee shops are separate entities whose proceeds help fund the services, can create awareness and lessen stigma around hospice care and are generally a cultural service which promotes community, conversation and fellowship.
|
|
Coffee & Tea Fundraisers
|
Ireland (http://www.marymount.ie/?page_id=5376)
|
The coffee and tea fundraiser run by the hospice was conducted throughout the city of Cork in many different venues, churches, halls, malls etc. They are informal and extensive events which engage the community in contributing to the hospice even if they themselves do not feel comfortable physically going to volunteer at the hospice.
|
|
Charity Shops
|
South Africa, Ireland, UK
|
Similar to coffee shops, charity shops or second hand shops, are another common area of social entrepreneurship where hospices and palliative care services are partially supported through the proceeds from the shop as well as creating an awareness of the services
|
|
Music Therapy
|
USA, Australia

|
Music therapists use music to engage with patients and their families. For patients with dementia, this can be an effective way to engage the mind. For others, it may be comforting, peaceful, another way to engage in holistic care for the entire person. (http://www.arttherapyblog.com/music-therapy/music-can-heal/#.V0XCnpD3arU)
|
|
Occupational Therapy
|
Australia, Canada, USA, UK and Ireland
|
This service is found in multiple capacities, both within the hospital or hospice in a gym or to work one on one with in patient patients. OTs also go to make house calls. Not only do they assist with managing muscle strength and creating a home environment which is better suited to a person with a particular illness, they are psychologically helpful due to the nature of their profession which takes an active hand in care giving.
|
|
Photography Programs
|
UK
|
Artistic photos of families and their loved one holding hands are presented to families after the passing of a loved one as a keepsake. In the UK, a photographer is hired by the hospital to carry this out in addition to other duties throughout hospital. (Though this could have a potential for a volunteer opportunity as well)
|
|
Day Care Services
|
South Africa, Ireland, the Philippines, Australia
|
Give a sense of purposefulness through a variety of activities such as crafting, getting hair and nails done, doing exercises, having a check up, having coffee and tea, reading the paper with volunteers and other patients etc. Services also provide respite for the family and engage volunteers in care. Depending on resources countries vary in programs.
|
|
Crèche
|
South Africa
|
Children in Johannesburg, South Africa can attend this Crèche if their parents are sick or receiving treatments, also open to others outside the hospice system to generate money
|
|
Wooden Holding Cross
|
UK

|
the wooden holding cross is designed to "fit comfortable into the palm of your hand during prayer and meditation, a holding cross can help ease the fears, worries and stress of children and adults alike, and help focus prayers. Also known as a Comfort Cross, because of the solace it offers to those using it, the Holding Cross is based on an ancient design found in a centuries-old European chapel." (www.holyroses.co.uk)
|
|
Reiki Therapies
|
USA, Japan
|
Reiki is an alternative "energy" therapy originating in Japan and there are a few studies in which it is shown to reduce anxiety and pain. (http://www.ncbi.nlm.nih.gov/pubmed/24582620)
|
|
Physiotherapy
|
USA, Canada, UK, Ireland, South Africa, Australia, Israel
|
having a Physio therapist or program as part of the holistic palliative service assists care in multiple ways. It can help to engage in one's care in an active way, even if the person cannot be cured, create a community when exercises occur in a gym where multiple patients can attend, assists in management of fatigue and breathlessness, having other staff monitor patient's progress, helps to improve mood, can be an introduction into a hospital if a patient is receiving home care at this time and could eventually need to move to an inpatient unit.
|
Education and Workshops
In meeting the needs of various communities, hospices and palliative care hospitals have developed classes, workshops and certificate programs to enhance the care and knowledge of their staff, volunteers and community members. Caring for the dying cannot be the sole responsibility of the health care system and by educating and equipping families, friends and communities, death and dying becomes a part of life, a time of growth and understanding.
One example of this emphasis on education is in South Africa, the opportunities were wide and diverse, providing the following courses in a separate building completely devoted to education:
1.Introduction to Palliative Care (palliative care theory, communication skills, breaking difficult news, symptom control, understanding symptom control, the role of psycho, social and spiritual care, the dying process)
2. Grief Loss and Bereavement Workshop (focus on hospice philosophy, self awareness, conceptualizing death and dying, understanding of mourning and bereavement)
3. 8 month (1 day per week) course in Palliative Nursing accredited by Hospice Palliative Care Association
4. Volunteer Course (knowledge and skills in field of grief, loss and bereavement, insight and understanding of patient and family affected by life threatening illness, interpersonal skills, self awareness, hospice philosophy)
5. Courses for the Carer at Home (focus on practical tasks of looking after a loved one or patient needing basic caregiving at home)
6. Physical Assessment Course (how to physically assess patient's needs, recording and assessing data, competency and correct use of anatomical landmarks to describe the site of the patient's signs and symptoms)
See here for more details or updates: http://hospicewits.co.za/training/
One example of this emphasis on education is in South Africa, the opportunities were wide and diverse, providing the following courses in a separate building completely devoted to education:
1.Introduction to Palliative Care (palliative care theory, communication skills, breaking difficult news, symptom control, understanding symptom control, the role of psycho, social and spiritual care, the dying process)
2. Grief Loss and Bereavement Workshop (focus on hospice philosophy, self awareness, conceptualizing death and dying, understanding of mourning and bereavement)
3. 8 month (1 day per week) course in Palliative Nursing accredited by Hospice Palliative Care Association
4. Volunteer Course (knowledge and skills in field of grief, loss and bereavement, insight and understanding of patient and family affected by life threatening illness, interpersonal skills, self awareness, hospice philosophy)
5. Courses for the Carer at Home (focus on practical tasks of looking after a loved one or patient needing basic caregiving at home)
6. Physical Assessment Course (how to physically assess patient's needs, recording and assessing data, competency and correct use of anatomical landmarks to describe the site of the patient's signs and symptoms)
See here for more details or updates: http://hospicewits.co.za/training/
Ethics & Issues
It is so important that you as medical professionals have at least a basic knowledge of the ethical consequences of the health care system and are able to reflect about the ethical aspects of your own personal caregiving. This reflection is helpful in terms of always rooting the care in the human being and not just his or her body.
On a very basic level assessing the following:
-What should we do? (What actions are good or right?)
-Why should we do it? (Exploring the reasons for our decisions.)
-How should we do it? (What plan is most ethical?)
*taken from the Hamilton Health Sciences "Ethics Consultation Service"
Further Practical Steps:
1. Recognizing that there is an ethical dimension
2. Break into component parts: a. Should or ought? b. Relevant principles at play (autonomy, veracity, beneficence, non-maleficence, confidentiality etc.) c. Acknowledge personal biases
3. Identify relevant facts: clinical evidence, quality of life assessment, context
4. Subject dilemma to critical analysis: examine values and identify conflicts, which values create obligations for you and to whom are they owed? Prioritization of values
5. Law and professional guidance: benchmark what is the current best practice? Consult with collegues. Know what is in the law.
6. Outcome: make and implement decision and be able to justify with solid arguments
*taken from ethics lecture given at Calvary Hospital, Sydney Australia
On a very basic level assessing the following:
-What should we do? (What actions are good or right?)
-Why should we do it? (Exploring the reasons for our decisions.)
-How should we do it? (What plan is most ethical?)
*taken from the Hamilton Health Sciences "Ethics Consultation Service"
Further Practical Steps:
1. Recognizing that there is an ethical dimension
2. Break into component parts: a. Should or ought? b. Relevant principles at play (autonomy, veracity, beneficence, non-maleficence, confidentiality etc.) c. Acknowledge personal biases
3. Identify relevant facts: clinical evidence, quality of life assessment, context
4. Subject dilemma to critical analysis: examine values and identify conflicts, which values create obligations for you and to whom are they owed? Prioritization of values
5. Law and professional guidance: benchmark what is the current best practice? Consult with collegues. Know what is in the law.
6. Outcome: make and implement decision and be able to justify with solid arguments
*taken from ethics lecture given at Calvary Hospital, Sydney Australia
|
For more resources on ethics click on the button below:
|
Three Wishes StudyOne of the most holistic and creative projects/studies, I encountered on my whole journey. This project worked to grant the last 3 wishes of a person dying in the ICU. It was transformative not only for patients, but their families and the staff. 100% worth the read and consideration when trying to improve one's own programs and caregiving.
Cook, Deborah, Marilyn Swinton, Feli Toledo, France Clarke, Trudy Rose, Tracey Hand-Breckenridge, Anne Boyle, Anne Woods, Nicole Zytaruk, Diane Heels-Ansdell, and Robert Sheppard. "Personalizing Death in the Intensive Care Unit: The 3 Wishes Project." Annals of Internal Medicine (2015)
|
The ETHICUS StudiesThese studies are informative for those not just in the ICU but in any realm of health care which deals with death and dying. recognizing that death is moving into the realm of health care and adjusting to the needs of the whole person during this delicate season of his or her life.
Sprung, Charles L., Paulo Maia, Hans-Henrik Bulow, Bara Ricou, Apostolos Armaganidis, Mario Baras, Elisabet Wennberg, Konrad Reinhart, Simon L. Cohen, Dietmar R. Fries, George Nakos, and Lambertius G. Thijs. "The Importance of Religious Affiliation and Culture on End-of-life Decisions in European Intensive Care Units."Intensive Care Med Intensive Care Medicine 33.10 (2007): 1732-739.
Sprung, Charles L., Thomas Woodcock, Peter Sjokvist, Bara Ricou, Hans-Henrik Bulow, Anne Lippert, Paulo Maia, Simon Cohen, Mario Baras, Seppo Hovilehto, Didier Ledoux, Dermot Phelan, Elisabet Wennberg, and Wolfgang Schobersberger. "Reasons, Considerations, Difficulties and Documentation of End-of-life Decisions in European Intensive Care Units: The ETHICUS Study."Intensive Care Med Intensive Care Medicine 34.2 (2008): 392-93.
|
|
More issues (ethical and other) to consider:
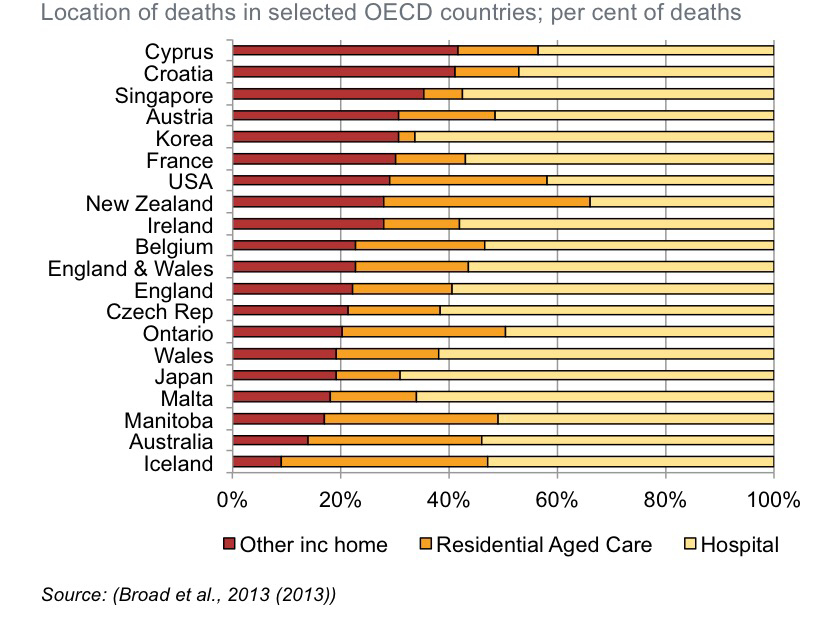
1. Majority of people want to die in their homes while the reality is that the minority actually do, in most 1st world countries (either die in nursing homes or hospitals). Point to consider: are the people we are surveying healthy when we ask them what are their wishes? Might these wishes change as people become more ill? Inpatient palliative and hospice units often have very positive feedback from patients and their families, perhaps the movement toward dying outside of the home is not completely a negative. (http://link.springer.com/article/10.1007/s00038-012-0394-5) 2. Wish: have end of life discussion during periods of medical stability vs. Reality: most take place in hospital triggered by acute medical crisis (Mack JW, et. al ANN Int Med, 2012) 3. Continuity of health care: does a specialist or primary care physician leave a patient hopeless or avoid difficult end of life discussions for someone else to take on? Why? Lack of education? Fear of discomfort? Questions to ask: what is the role of honesty? Can conversations occur gradually over a certain period of time? How are disciplines collaborating and communicating to best help the patient and keep care from becoming disjointed? 4. Do you as a medical provider understand the importance of Advanced Directives? Are they important? Why or why not? 5. Is there mutual respect between disciplines? Between hospitals? Some countries have great continuity between hospitals and even rely on each other's specialties for consulting. Others are very disjointed. This can be due to hypercompetitive culture or lack of resources. 6. Withholding or Withdrawing treatment is a huge ethical issue. Israel has a particular law in place, Halacha Law, which prevents the withdrawal of ventilator once a person is reliant upon it for life as a reflection of religious teaching, in other cultures, this stance is not so black and white and must be discerned with great care and discretion. 7. Euthanasia and Physician Assisted Suicide (Dying) are two huge ethical topics in end of life care. Though outlawed in most of the world, countries like Belgium and the Netherlands ((B) in law 28 March 2002, took effect 3 Sept 2002 The Belgium Act on Euthanasia; (N) in law: 10 Apr 2001, took effect: 1 Apr 2002 Termination of Life on Request and Assisted Suicide Act) have legalized euthanasia. A few states in the US, such as Oregon and California have legalized physician assisted suicide ((OR) in law: 8 Nov 1994, take effect: 27 Oct 1997 Death With Dignity Act; (CA) in law: 5 Oct 2015 , take effect: 9 June 2016, End of Life Option Act) through argument that one should have the right to "choose." The difference as stated in the definitions portion as to the level of involvement of the physician, if (s)he is administering the drugs or simply prescribing and the autonomous person consuming or injecting them. Most palliative and hospice care professionals specifically and associations have made public statements against euthanasia and PAS as undermining their care as palliative teams. Their purpose is to manage pain and allow for natural death not to hasten death nor lengthen life. Point to ponder: is the "choice" to die ever completely independently made? What other influences are at work? Does fear play a part? What about the feeling of being a burden? |
Image taken from: Swerissen H., Duckett S. Dying Well (2014) http://grattan.edu.au/wp-content/uploads/2014/09/815-dying-well.pdf
8. Decisions around narcotics and resources also cause ethical issues. Certain narcotics, if taken in extreme can hasten death but in balance can lead to better quality of life and thus must be adequately monitored. However restrictions regarding these medications can cause harm when persons live in areas with scarce resources or in difficult to get to locations such as in the islands of the Philippines where restrictions on the distributions on medications cause many people to forego accepting any pain reducing drugs for fear that they might not be able to get them the next time they need them and would thus rather adapt to the pain than address it.
9. Ethical distribution of organs for transplants is a problem around the world with the lack of needed organs as well as cultural values and stigma around donating one's organs. 10. Principle of Double Effect: giving medication with the purpose of relieving pain in order to provide comfort is morally acceptable even if as an unintended side effect death is hastened to a degree 11. Hoping for the best but preparing for the worst is a good way to approach difficult discussions around terminal illness 12. Being aware of cultural issues is important and it is always better to ask than to make assumptions about care |
Bereavement Services Around the World
|
Faith and Spirituality |
|
Australia- counseling services, support groups and workshops, education and training on grief, loss and bereavement to health professionals, consultation to the general public and health professionals as requested. Self referral service.
"On Death and Dying" by Elizabeth Kubler-Ross of Switzerland provides great insight into loss and grief 
|
Recognition that particularly during the conversations and care around end of life, there are many personal, existential questions around one's life and his or her purposefulness, why he or she is on this earth, what he or she brought to the world is of great importance in your role as caregiver. To ignore this element of a person's identity is to neglect the whole-ness of that person.
An awareness of spirituality and religious perspectives can give a great deal of insight into one's feelings and choices around organ donation. (www.donatelife-pa.org) Many hospice organizations were originated by religious groups or orders and though they may no longer be associated with those groups, the ethos often remains. It is frequently the case that patients express caution because they are afraid that the groups will try to convert them while providing care or will not provide as good of care if they are not of that same faith. Generally this is not the case. The commitment to provide quality health care, in so far as it is available in each culture, is generally the priority and if the person desires to engage in a faith on a deeper level, they are very welcome to avail of this, but it is not forced. This was the case in the UK, Ireland, Australia and India. In fact, most hospices and palliative care hospitals have their own websites outlining thief mission, philosophy and ethical codes. As a health care professional, it is good to be aware of basic values that each faith holds, while recognizing that people practice their faiths differently and therefore inquiring about their decisions and choices is of the utmost importance. For a resource on faith traditions: (http://inclusion.infonet.upmc.com) |
VolunteerismVolunteer engagement in hospice care and in hospitals varies around the world but always engages communities, helps to increase awareness of issues, provides skill sets, knowledge and understanding even on a basic level for being able to handle and cope with death and dying in loved ones' lives and in one's own life.
Hear are some ideas from around the world of engaging the volunteers... 1. No One Dies Alone Program (Pittsburgh, USA): This program trains volunteers to sit with patients in the hospital who might not have family or friends nearby to sit with them in their last moments to "have the gift of human presence in their final hours." 2. Day Care Programs (Cork, Ireland; Sydney, Australia; Los Banos, Philippines; Johannesburg, South Africa): Day care programs bring members of the community into engaging activities with patients in hospice or palliative care. These services can bring in skilled workers such as hair stylists or massage therapists or just members of the communities to work on crafts, have tea and coffee and just spend time with patients in a welcoming environment. Not only does this benefit patients and volunteers but also provides some respite for family members and primary care givers. 3. Education and training (USA, Canada, Ireland, South Africa, Australia): different cultures have different requirements for training depending on the culture. As this is a sensitive subject, more extensive training than for volunteers in other aspects of health care often occurs. Training on ethical issues, basic understanding of palliative and hospice care, self care assessment and avenues for reflection all foster sustainable and fruitful volunteerism and holistic care for patients and their families. |
  |
Importance of Space and Design
Dear medical professionals, place yourselves in the shoes of your patients. You in a hospital bed or an in-patient unit. What does the room look like? If you were in perfect health, would lying in this bed be stressful? Now add on being ill. Are there 20 doctors in white coats standing around you, discussing you? Are you adequately covered or are festering body parts out in the open for all eyes to see? Is there a constant buzzing from different machines, not just in your room but in surrounding rooms? Do the lights overhead hurt your eyes and prevent you from being able to sleep? Are the walls bright, clinical white or yellow? Are you comforted by this? If you were treated by your doctor the way you treat your patients, how would you feel? What about the family? Are you having difficult discussions with them in a hallway, standing up or in a separate, private room, sitting down? How does that change how the information is presented and received?
Sometimes we get so caught up in the really difficult, medical aspects of care, we forget that such small simple things like the paint color on the walls or completely covering a person or only allowing one or two doctors in a room at a time so as not to overwhelm a patient, make an enormous difference. Details matter for human beings.
Sometimes we get so caught up in the really difficult, medical aspects of care, we forget that such small simple things like the paint color on the walls or completely covering a person or only allowing one or two doctors in a room at a time so as not to overwhelm a patient, make an enormous difference. Details matter for human beings.






